|
I don’t really think anything is ever black and white, completely good or completely bad. My latest CT scan, for example, was a mixed bag of news, even significant and insignificant. In a way, this helps me prepare for scans in general, if I believe that there won’t really be any extremes, or anything too shocking or groundbreaking. And then if there is, I get to be pleasantly surprised (or maybe unpleasantly blindsided, and I’ll cross that bridge if I come to it).
The bad news on my latest scan is that the FOLFIRINOX didn’t really work, all of my “drop metastases” grew, my pancreatic pseudocysts grew, and I have a small pulmonary embolism (a blood clot in my lower left lung). Also, according to my latest lab tests, my tumor marker number has risen again, to the 150’s. The good news is that my original tumors (pancreas and liver) are relatively stable, and my doctor thinks it’s time to try experimental treatment, which means immunotherapy. Sometime last year, another CT scan revealed a few different bits and pieces of “worsening metastatic disease,” as my cancer grew and spread. I had and/or have ascites (extra fluid in the abdominal cavity), carcinomatosis (general systemic spread of carcinoma cancer cells), and “nodules,” or tiny little extra tumors floating around in my abdomen. Later on, these nodules started to land in various places and attach themselves to various parts of my insides. As of this latest scan, these nodules, now called “drop metastases” because they’ve literally dropped within my insides due to gravity, have all landed somewhere in my pelvic region, and they’ve all grown. One of these tumors is now 7.5cm in one direction (roughly the size of a clementine?) and is pressing on my bladder. Others are “likely ovarian metastases.” I don’t honestly know whether this means that I now have cancer in my ovaries, or if it’s just little bits of extra cancer on and around my reproductive organs, not necessarily affecting any organ function. Maybe I don’t really want a definitive answer to that question. Regardless, I’m not having any significant symptoms yet from any of these drop metastases, just occasional pelvic pain (like ovulation cramping, which most ladies will understand). And regardless, these extra little cancer bits are raising some complex psychological issues for me, the kinds of conflicting thoughts and worries that I imagine women with reproductive cancers face regularly. And also, I’ve had increased pancreas pain, probably from the growth in the pseudocysts (cystic lesions with a different density and makeup than typical cysts) surrounding my pancreas tumor. All of that means that while the FOLFIRINOX chemo cocktail worked fine on my pancreas and liver tumors, it kind of did diddly squat on a systemic level, allowing these drop metastases to grow way too fast. So David and I crawled through hell four times (those four rounds of FOLFIRINOX), and for what? We’re still here, on the other side, at least. The pulmonary embolism is a surprise. Apparently, though, this happens a lot with pancreatic cancer, which thickens the blood. Fortunately, this one is still quite small, which means we caught it early. The radiologist called my oncologist immediately after the scan, before my clinic appointment, to notify him, so that’s a bit alarming. My oncologist said that while it’s urgent and potentially life-threatening, it’s also very treatable. All I need to do is twice daily shots of heparin (an anticoagulant) for a month, then blood thinner pills for a while. I haven’t had any symptoms from it yet either, which is a good sign. Although now I find myself overthinking my usual breathing patterns, wondering if what I’m feeling any given moment is shortness of breath or not. So far, the shots are going fine. They were icky at first, like the Neupogen shots I’ve done before, with a thick needle on the syringe that doesn’t push into my belly skin very easily. But lately they seem to have gotten easier. I’m about halfway through my month of shots, and I look forward to the end of this chore every 12 hours, and even to the end of the twice daily reminders that pop up on my phone. The positive outcome of this scan is that I finally get to try immunotherapy! I’ve been asking my oncologist about this every clinic visit, and he finally suggested it himself. Now is the right time, because I’ve tried a year of two different chemo regimens. While the first one was very successful initially, this traditional systemic treatment hasn’t been effective enough for me in general. Also, apparently in the last few months, the number of available immunotherapy clinical trials for pancreatic cancer has grown significantly, and there are several new ones at Johns Hopkins itself. David and I researched through the PANCAN clinical trials database and carefully considered our options (at a few Baltimore hospitals, as well as NIH in Bethesda, MD, Georgetown in DC, and Penn in Philadelphia). While we found one we really like at NIH (which I’d prefer to do first, for a variety of reasons), I wouldn’t qualify for our top choice trial at Hopkins if I did this NIH one first. So we decided to go for the Hopkins trial now, and my oncologist is coincidentally the principal investigator. I will hopefully start the screening and enrollment process this week, then start the actual treatment within two weeks from that date. Then it’ll be three weeks on, one week off, with a combination of immunotherapy pills (Palbociclib) and one short weekly chemo infusion (Abraxane). I was hoping to avoid any chemo for a while and do an immunotherapy-only trial, but it seems I might have trouble qualifying for those, because I already have an autoimmune condition, type 1 diabetes. So my hair might fall out again (in which case I think I’ll try out a wig), or it might continue to grow in, which would be a lovely surprise. (I almost have an even buzz cut of new growth now, with this break from treatment.) Fortunately, because I’ll be doing only one chemo drug (as opposed to three or four, as with my previous treatments), the side effects should be pretty manageable. Unfortunately, clinical trials are quite time-intensive and run on regimented schedules, so I won’t have the flexibility I’ve had so far, and I won’t be able to tailor my treatment schedule to my work schedule. We’ll see how it all works out. So for now, we are cautiously optimistic. Immunotherapy is incredibly promising and exciting, the forefront of cancer research and the closest science has come to a cure. In fact, a good friend of mine who works in a cancer research lab and is currently taking a graduate course on advanced cancer biology, just told me yesterday about her professor’s astounding success treating APL leukemia. He’s achieving a 96% complete response (“no evidence of disease,” which is virtually a total cure) in his patients, treating them with high doses of vitamin A (the immunotherapy component) and tiny doses of arsenic (the systemic toxin, or chemotherapy component). These results are absolutely staggering, especially for a cancer that has been notoriously difficult to treat. Of course, all pancreatic cancer, and mine in particular, is generally resistant to treatment, and so far, researchers have not had the same success with immunotherapy for pancreatic cancer that they’ve had for other cancers. But my oncologist did say that research so far has shown that patients who are treated with both Palbociclib and Abraxane have better outcomes than those who are treated with either drug individually. It’s certainly worth a try. As always, I’m consciously working on remaining mindful in the present moment, detaching myself from worries and expectations about the past or the future, and hoping for the best while preparing for the worst. This is the healthiest, most comfortable approach for me, so I’m sticking with it. One day at a time.
2 Comments
Tomorrow, January 21, 2017, hundreds of thousands of people are expected to participate in the Women's March on Washington, D.C., not to mention the countless others participating in local marches around the country. The mission of the Women's March inspires me: "We stand together in solidarity with our partners and children for the protection of our rights, our safety, our health, and our families - recognizing that our vibrant and diverse communities are the strength of our country." Unfortunately, because of my health, I cannot physically attend any of these protest marches, either in D.C. or in my own city of Baltimore. As much as I would love to be there in person, I cannot manage the travel, mobility, weather, crowds full of germs, risk of teargas and other chemical attacks, and long hours. Fortunately, though, there is the Disability March. Founded by a group of people with disabilities and chronic illnesses, as well as disability allies, the Disability March is a virtual protest in solidarity with all of the physical Women's Marches happening tomorrow. The Disability March is a co-sponsor of the national Women's March, and it allows those who cannot attend a protest in person to participate in the movement. If, like me, you cannot get to the march in the nation's capital or even in your own local city or town because of disability or chronic illness, I encourage you to join the Disability March online. Email [email protected] with the following information, including a photo attachment, by the end of the day today. Then watch the site for your post to appear as the organizers publish the many entries they receive. Share your post, and this virtual solidarity movement, on social media and by word of mouth.
Challenging times are ahead. Our incoming president has mocked people with disabilities, ignored our rights and value, and pledged to decimate public services for people with disabilities and chronic illnesses. We cannot allow this new president to steal our futures. If we are silent, we are complicit in the damaging lie that we are worthless, or worthy only of dismissal and mockery. We must stand up for ourselves, our rights, and our dignity. Join me in this movement. Disability rights are human rights, and human rights are disability rights. 
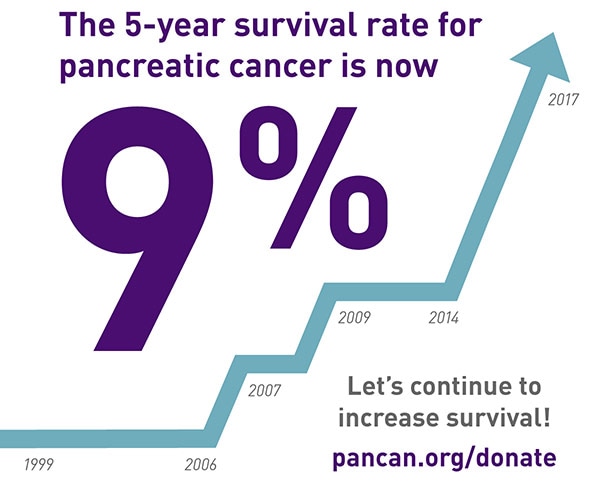
In your first five years of living with cancer, numbers matter. Statistics inform your treatment, your doctor's recommendations, your prognosis, your mood on any given day, and your chances for the future. At the same time, statistics mean absolutely nothing because every individual cancer is independent and unique, and many people defy statistics. Also, if you have a particularly rare form of cancer (or a rare case of a relatively rare cancer, like I do), the shape and path of your cancer is likely not reflected at all in current research. Maybe your case will contribute to research, but that means that the numbers you’ll be able to find (or the numbers your doctor might, eventually, reluctantly reveal to you) really don’t apply to your case at all. You find yourself surrounded by numbers, some encouraging and some decidedly terrifying, but unable to reach out and hold onto to any of them, because there’s a very real chance that not a single one of them matters to your life. This has been my relationship to pancreatic cancer statistics over the last year. I have sought them out, because I’m a naturally curious person, and because I found early on that the more information I had about my new medical reality, the calmer and more confident I felt. I have used them to explain my situation to others, and I have used them to lobby Congress for pancreatic cancer research funding. It is certainly compelling to state dramatically that my cancer, stage IV pancreatic cancer, has a five-year survival rate of only 1%. However, I know that I cannot put any stock in these numbers. Both because they may not be accurate for my particular case, and because putting stock in these statistics is dangerous for my mental health. I can’t let myself think much at all about the possibility that I have only a 1% chance of living to see 2021. I can’t let myself imagine the chance that I might not live to age 35, or celebrate my 7th wedding anniversary, or attend any college reunions past my 10 year. I also can’t let myself worry that I might be in cancer treatment for the rest of my life, or that I’ll never get to have a child, or that I might never be able to get rid of my pancreas and thus slough off this burden that’s weighing me down from the inside. But of course, I do think about all these horrible possibilities. I think about them all the time. Recently, my therapist asked me for a clarifying example when I mentioned that I’ve become much more conscious of my own mortality since my last CT scan, in October, which revealed that my first chemo regimen had stopped working and all of my tumors were growing. I told her that whenever I enter recurring dates in my work calendar, such as my story time assignments on our rotating department schedule or my monthly committee meetings, I find myself casually thinking, oh, might not make it to that one, or I wonder if I’ll still be alive then. These aren’t always negative thoughts, in fact, they’re often neutral, nonchalant musings. It’s not so much that I’m upset by those low-single-digit percentages in all the statistics, but rather that they are the context for how I think about nearly every aspect of my life now. When I make plans for the future, or consider my priorities, or imagine how my life might change over the years, I am always conscious of that five-year frame around my future. In a sense, it has shrunk my perspective down to a smaller box, in which every small thing becomes larger by comparison, and the things that really matter glow so much brighter than they used to. Really, this smaller perspective on the entire span of my life makes it much easier to see quickly what truly matters to me. I don’t have to fumble anymore to figure out my priorities, and it’s easier for me to drop and walk away from the things that don’t make a difference to me in the long run. Because I may not have a long run. In some recent FMLA paperwork that my nurse practitioner filled out for my husband and me, she listed my prognosis as “guarded” and my typical recovery period as “lifelong.” Those two little words can definitely make you stop and clarify your priorities pretty quickly. As I head into what will surely be a telling CT scan on Wednesday (the first since starting my new chemo regimen), I too am guarded. But I’m also living mindfully, cherishing every little moment of my lifelong. |
Authorchildren's librarian, Smithie, writer, reader, cook, gardener, cancer patient, medical oddity, PANCAN patient advocate, #chemosurvivor, #spoonie Categories
All
Archives
January 2017
|
 RSS Feed
RSS Feed